
Understanding New Health Equity and Quality Requirements for California Health Plans
Starting in 2023, systematic data collection and reporting of health equity and quality measures are required of all full-service and behavioral health plans licensed by California’s Department of Managed Health Care (DMHC).

There is growing recognition that standardized, high-quality data is increasingly critical to drive improvements in health equity. In California and nationwide, momentum is building to adopt standard health equity and quality measures to improve the equitable delivery of high-quality healthcare services.
DMHC Health Equity and Quality Requirements
Starting in 2023, systematic data collection and reporting of health equity and quality measures are required of all full-service and behavioral health plans licensed by California’s Department of Managed Health Care (DMHC). DMHC also requires plans to stratify the data reported by race and ethnicity using the National Committee for Quality Assurance’s (NCQA) race and ethnicity methodology, aligned to the federal Office of Management and Budget standards for stratification.
This new requirement is the output of the work completed by DMHC’s Health Equity and Quality (HEQ) committee following the passage of Assembly Bill 133 (AB 133) in 2021. The bill required the DMHC to convene the HEQ committee to recommend health equity, quality measures, and benchmark standards for all health plans. The committee’s goal was to address long-standing health inequities and work toward achieving more equitable delivery of high-quality healthcare services across all market segments, including the individual, small and large group markets, and Medi-Cal managed care plans.
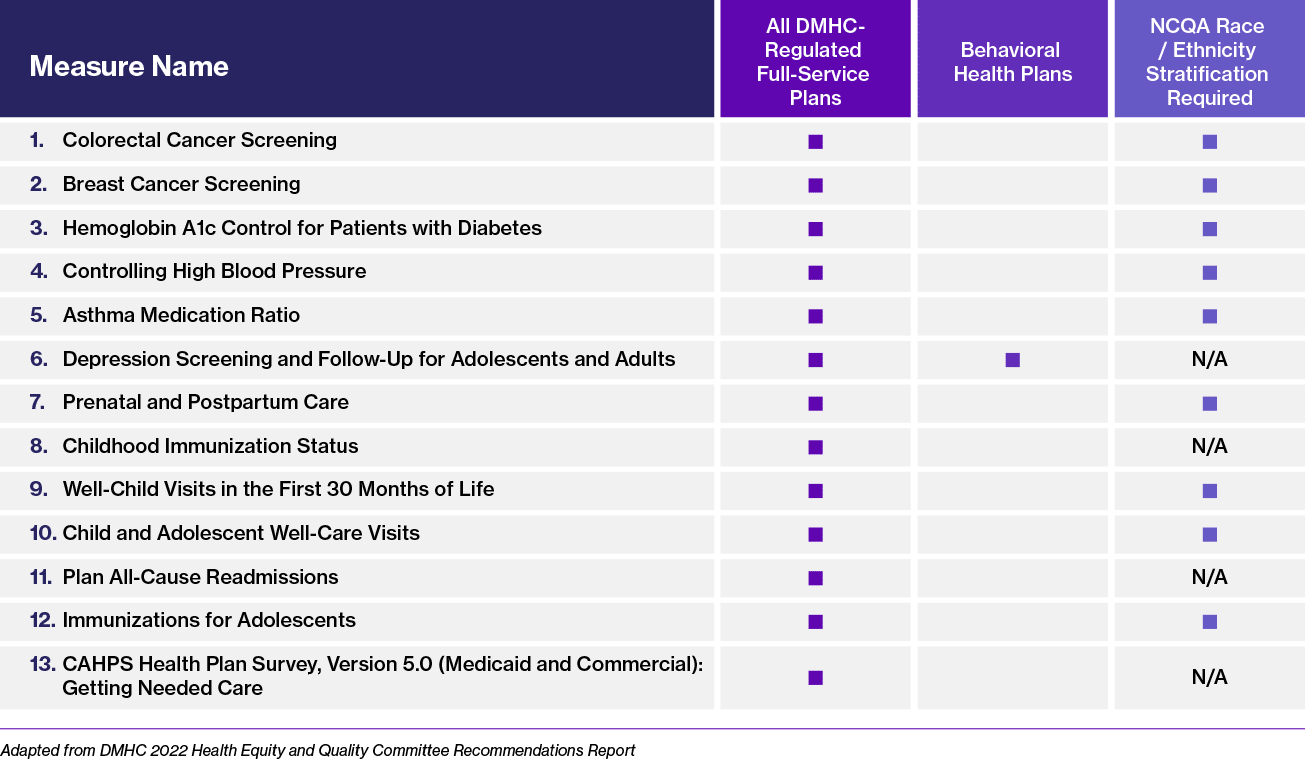
In October 2022, the DMHC accepted from the HEQ committee its final recommendations for a Health Equity and Quality Measure Set (HEQMS) and stratification requirements comprising the 12 measures (from the Healthcare Effectiveness Data and Information Set®) and one Consumer Assessment of Healthcare Providers and Systems (CAHPS®) measure. As the table below summarizes, all DMHC-licensed full-service health plans are to report on all HEQMS measures in Measurement Year (MY) 2023. Behavioral health plans must report only on HEQMS measure #6, “Depression Screening and Follow-Up for Adolescents and Adults.” Nine of the 13 HEQMS measures are to be stratified by race and ethnicity, per NCQA standards.
Is It Time To Do More With Your Health Equity Programs?
Learn more about Freed’s health equity consulting services to see how Freed helps organizations achieve measurable impact toward eliminating disparities.
DMHC Health Equity and Quality Measure Set
Applicable measures by plan type and stratification by race and ethnicity.
Benefits of Standardizing Healthcare Data Collection
Standardized high-quality data collection is not only a pre-requisite to understanding underlying barriers to access, outcomes, and affordability, but is essential for:
- Identifying health disparities at the population level,
- Uncovering interrelated social determinants of health (SDOH) factors contributing to health inequities,
- Guiding investment priorities both in the design and implementation of targeted interventions, and,
- Facilitating impact measurement against standard benchmarks to help achieve greater health equity.
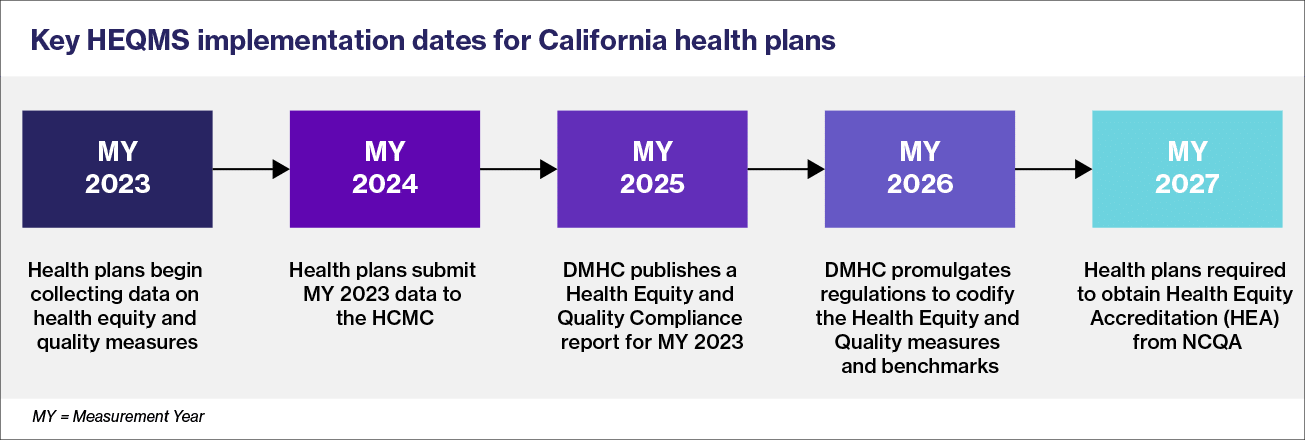
California’s DMHC Data Reporting Timeline
Health plans are well into their data collection cycle for MY 2023, which will be followed by reporting of this data to DMHC in 2024. The DMHC will then begin publishing a Health Equity and Quality Compliance Report on the data and information reported by health plans starting in 2025. Per DMHC guidelines, the HEQMS data collection and reporting will run through MY 2023 through at least MY 2027. After five years, the DMHC may reconvene the HEQ committee to adjust or revise the HEQMS. (Refer to the key implementation milestones below).
The DMHC’s HEQMS reporting requirements are not entirely new to health plans. Most plans are already reporting against a number of the performance measures, as a condition of their participation in various value-based programs. Because the new HEQMS requires stratification by race and ethnicity, health plans will derive even greater insights from gaps in outcomes. In turn, this will help direct their efforts toward prioritizing quality improvement programs to specific patient population segments, enhancing service delivery models and facilitating robust patient engagement.
DMHC’s HEQMS provides a solid foundation to expand and align with emerging state and national initiatives toward reducing disparities and inequities in health care. When viewed as not just a requirement, but also as an opportunity for improvement, health plans can make significant progress toward establishing more patient-centric, equitable care.



